Roughly 4 million Americans live with fibromyalgia — a condition defined by widespread musculoskeletal pain, crushing fatigue, disordered sleep, and cognitive fog that conventional medicine still struggles to fully address. For many patients, cannabis fibromyalgia relief has moved from anecdote to active investigation, with multiple clinical surveys now reporting meaningful symptom reduction across pain, sleep, and mood domains.
This guide goes deeper than a simple strain list. We break down the neurological mechanisms that make fibromyalgia uniquely responsive to cannabinoids, explain which cannabinoid ratios and terpene profiles target each symptom cluster, and match those profiles to real strains you can actually grow or source.
What Fibromyalgia Actually Does to the Nervous System
Cannabis works best for fibromyalgia when you understand why the condition is so difficult to treat. Fibromyalgia is not simply chronic pain — it is a disorder of central sensitization, where the brain and spinal cord amplify pain signals far beyond any detectable tissue damage.
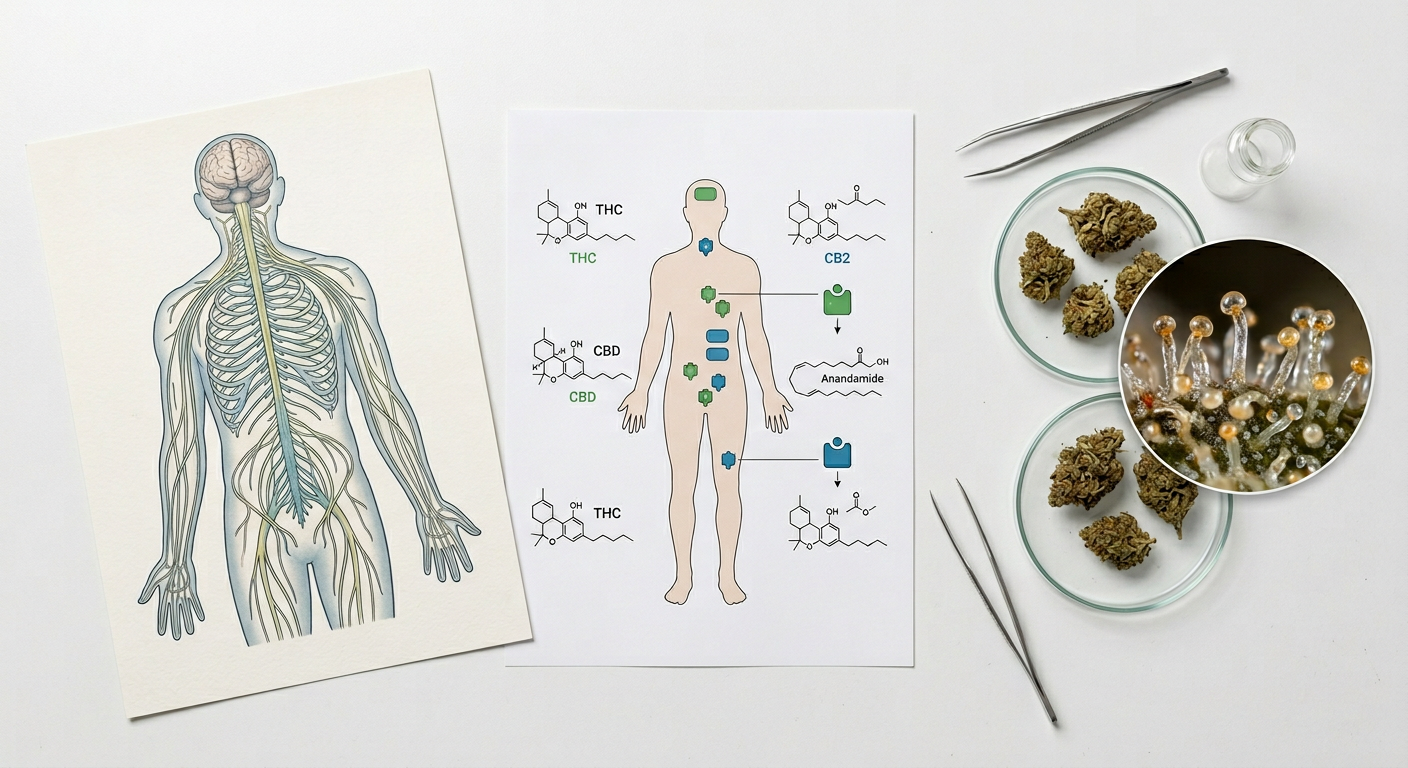
Fibromyalgia pain arises from dysfunction in the body's own pain-modulation systems, including the endogenous opioid and endocannabinoid pathways. Research published in PLOS ONE (2016) proposed that fibromyalgia may partly reflect Clinical Endocannabinoid Deficiency (CECD) — a state where the body produces insufficient endocannabinoids to regulate pain, sleep, and mood.
Endocannabinoid Deficiency Hypothesis: Dr. Ethan Russo's CECD theory (2004, updated 2016) suggests fibromyalgia, migraine, and IBS share a common thread — underactive endocannabinoid tone. Exogenous cannabinoids like THC and CBD may compensate directly by binding CB1/CB2 receptors and modulating the same pathways that fibromyalgia disrupts.
The three major symptom clusters in fibromyalgia are:
- Widespread pain and allodynia — pain from stimuli that shouldn't hurt (light touch, clothing)
- Non-restorative sleep — particularly disrupted slow-wave (Stage 3) sleep
- Cognitive impairment and mood dysregulation — often called "fibro fog"
Each cluster responds to different cannabinoid and terpene combinations, which is why choosing the right strain matters far more for fibromyalgia than for many other conditions. A daytime energizer that helps mood may shatter nighttime sleep; a heavy sedative may worsen morning fog.
Fibromyalgia Cannabis Research: What the Studies Actually Show
Published fibromyalgia cannabis studies now offer enough data to move beyond anecdote. The most important findings show measurable improvement in pain intensity, sleep quality, and patient-reported quality of life — though effect sizes vary considerably by dose and cannabinoid ratio.
A landmark 2018 observational study from Israel's Rabin Medical Center followed 367 fibromyalgia patients using medical cannabis for 6 months. Results showed 81% reported significant pain improvement, over 50% reduced or discontinued opioid use, and 73% reported improved sleep quality. Mean pain scores dropped from 9.0 to 5.0 on a 10-point scale.
A 2019 Israeli fibromyalgia cannabis study found that patients using inhaled cannabis had faster onset of pain relief (within 30 minutes) compared to oral preparations, while oral CBD-dominant products provided longer-lasting sleep benefits lasting 4–7 hours. Delivery method matters as much as strain choice.
Key findings from the published fibromyalgia cannabis study landscape include:
- Skrabek et al. (2008): Synthetic THC (nabilone) significantly reduced pain and fibromyalgia impact scores vs. placebo in a double-blind RCT
- Habib & Artul (2018): 81% of patients reported improvement; opioid use dropped by 50%+ in over half of participants
- van de Donk et al. (2019): Vaporized cannabis with balanced THC:CBD produced the greatest analgesic effect in a crossover trial
- NIDA review (2021): Noted consistent but moderate evidence across observational data; called for controlled trials
Research Gap Alert: Most fibromyalgia cannabis studies are observational, not randomized controlled trials. Effect sizes may be inflated by expectation bias. Current evidence strongly justifies patient trials under medical supervision, but does not yet confirm optimal protocols.
The consistent theme across these fibromyalgia cannabis studies is that balanced THC:CBD ratios outperform either cannabinoid alone for pain, while CBD-dominant preparations show stronger benefit for anxiety and sleep maintenance. See our guide on the entourage effect for why this makes biochemical sense.
THC vs. CBD for Fibromyalgia: Mechanisms & Roles

THC and CBD play distinct but complementary roles in fibromyalgia symptom management. Understanding their individual mechanisms helps you choose the right ratio for each time of day and each symptom cluster — not just the highest THC number on a label.
How THC Addresses Fibromyalgia Pain
THC binds directly to CB1 receptors concentrated in the brain's pain-processing regions — the periaqueductal gray, thalamus, and anterior cingulate cortex. This is the same pathway disrupted in central sensitization. THC essentially turns down the amplifier that fibromyalgia has turned up.
THC also promotes slow-wave sleep, the deep restorative stage that fibromyalgia patients are systematically deprived of. Research shows low-dose THC (2.5–5 mg) increases Stage 3 sleep duration without significantly suppressing REM sleep — a critical distinction from prescription sleep aids.
Caution — THC Sensitivity in FM: Fibromyalgia patients frequently report heightened sensitivity to THC, especially at high doses. Starting above 10 mg THC can trigger anxiety, tachycardia, and paradoxical pain amplification in some patients. Begin at 2.5 mg and increase by 2.5 mg increments no sooner than every 3 days.
How CBD Addresses Fibromyalgia Symptoms
CBD does not bind strongly to CB1/CB2 receptors. Instead, it modulates the endocannabinoid system indirectly by inhibiting FAAH, the enzyme that breaks down anandamide — the body's own "bliss" endocannabinoid. Higher anandamide levels may directly address the CECD hypothesis underlying fibromyalgia.
CBD also interacts with serotonin 5-HT1A receptors and TRPV1 channels, both implicated in pain sensitization and mood regulation. A 2019 review in Frontiers in Pharmacology identified CBD's anti-inflammatory, anxiolytic, and sleep-modulating properties as specifically relevant to fibromyalgia's multi-system dysfunction.
Optimal Cannabinoid Ratios by Symptom
| Symptom | Recommended Ratio | Timing | Notes |
|---|---|---|---|
| Widespread pain (daytime) | 1:1 CBD:THC | Morning / midday | Functional relief without heavy sedation |
| Allodynia / touch sensitivity | 2:1 CBD:THC | As needed | Topicals also effective for localized areas |
| Sleep onset difficulty | 1:2 CBD:THC | 60–90 min before bed | Indica-dominant strains preferred |
| Sleep maintenance (waking at night) | CBD-dominant (4:1+) | Before bed, oral | Longer duration than inhalation |
| Fibro fog / cognitive symptoms | High CBD, minimal THC | Daytime | Avoid high THC — worsens cognition |
| Mood / depression symptoms | 1:1 or sativa-leaning THC | Morning | Limonene-rich strains amplify effect |
Terpene Science: The Hidden Factor in Fibromyalgia Strain Selection

Terpenes are the aromatic molecules that give each cannabis strain its distinctive smell — and they do far more than scent. In the context of weed fibromyalgia pain relief, specific terpenes modulate the analgesic, sedative, and anxiolytic effects of cannabinoids in ways that can make or break a strain's usefulness for FM patients.
The most therapeutically relevant terpenes for fibromyalgia target the same neurological systems the condition disrupts: serotonin signaling, GABAergic inhibition, inflammation cascades, and opioid receptor activity.
Key Terpenes for Fibromyalgia
- Myrcene — The most common cannabis terpene. Sedating, muscle-relaxing, enhances THC penetration through the blood-brain barrier. Dominant in OG Kush, Northern Lights, Purple Kush. Critical for pain and sleep.
- Linalool — Found in lavender and select cannabis strains. Activates GABA-A receptors, producing anxiolytic and sedative effects without THC. Directly relevant to fibromyalgia's anxiety and sleep components.
- Caryophyllene — The only terpene that directly binds CB2 receptors. Acts as a non-psychoactive cannabinoid, reducing neuroinflammation and peripheral pain signaling. Abundant in OG Kush, Cookies strains.
- Limonene — Citrus-forward, elevates mood via serotonin and dopamine pathways. Counteracts depression and anxiety that frequently accompany fibromyalgia. Strong in Sour Diesel, Super Lemon Haze.
- Pinene — Acts as an acetylcholinesterase inhibitor, potentially counteracting short-term memory impairment from THC. Especially valuable for fibro fog. See our complete pinene guide.
- Humulene — Anti-inflammatory, acts on CB2 and TRPV1 receptors. Adds appetite suppression (useful for FM patients managing weight). Covered in depth in our humulene terpene guide.
Terpene Preservation Tip: Fibromyalgia patients relying on terpene-driven effects need properly cured cannabis. Rushed drying destroys linalool and limonene fastest — cure at 58–62% relative humidity for a minimum of 4 weeks to preserve full terpene expression. See our drying and curing guide.
Best Strains for Fibromyalgia: Pain, Sleep & Mood Profiles

The best marijuana strains for fibromyalgia address multiple symptom clusters simultaneously. Each strain below is selected for its specific cannabinoid-terpene profile, not just raw THC content — and matched to the FM symptom it targets most effectively.
For Nighttime Pain & Sleep: Heavy Indica-Dominant Strains
Cannabis fibromyalgia sleep improvement requires strains rich in myrcene and linalool with moderate-to-high THC to promote slow-wave sleep architecture. The following deliver sedating, full-body relaxation without aggressive cognitive distortion.
Purple Kush — The Sleep Specialist
Purple Kush Feminized Seeds (27% THC) is a pure indica from Hindu Kush genetics, producing exceptionally heavy myrcene and linalool expression alongside its high THC ceiling. Its body-melting stone directly targets allodynia and the hyperalgesic pain spikes that spike at night in FM patients.
- Best for: Severe nighttime pain, sleep onset failure, restless legs in FM
- Dose guidance: 2–3 puffs vaped at low temp (170°C) 60 min before bed
- Caution: 27% THC is high for FM-sensitive patients — grow from seed and harvest at peak amber trichomes (30–40% amber) for more CBN and deeper sedation
Northern Lights x Big Bud — Broad-Spectrum Relief
Northern Lights x Big Bud Feminized Seeds (20% THC) combines the legendary analgesic body-load of Northern Lights with the generous terpene production of Big Bud. THC is more approachable at 20%, making it better suited for FM patients who find Purple Kush overwhelming.
- Best for: Whole-body pain relief, sleep maintenance, FM patients new to high-THC strains
- Terpene profile: Myrcene-dominant with earthy caryophyllene — anti-inflammatory and sedating
Skywalker OG Autoflower — Accessible Fast-Grow Option
Skywalker OG Autoflower Seeds (23% THC) deliver OG Kush's caryophyllene-dominant analgesic profile in an autoflowering format that reaches harvest in 75–80 days. For FM patients who want to grow their own consistent medicine supply, autoflowers remove the photoperiod complexity entirely.
Growing your own fibromyalgia cannabis gives you complete control over harvest timing, terpene preservation, and cannabinoid profile — all of which directly impact therapeutic outcomes. Harvesting when 30% of trichomes show amber coloration increases CBN content, amplifying sedation for sleep applications.
For Daytime Pain Without Sedation: Balanced & Sativa-Leaning Strains
Weed fibromyalgia pain management during waking hours requires strains that reduce pain intensity without compounding fibro fog or inducing sedation that interferes with daily function. Limonene and pinene-rich strains with moderate THC (18–22%) strike this balance most reliably.
Sour Diesel — Functional Daytime Analgesia
Sour Diesel Feminized Seeds (24% THC) is arguably the most functional daytime strain for FM patients. Its dominant terpene profile — limonene, caryophyllene, and myrcene in that order — produces energized pain relief with an anti-depressant lift that directly targets fibromyalgia's mood and motivation components.
- Best for: Morning pain, mood elevation, combating fibro fog fatigue
- Avoid if: Anxiety is a major symptom — sativa-dominant strains can amplify anxious thought loops in some FM patients
- Terpene advantage: Limonene's serotonergic activity adds genuine antidepressant effect alongside pain relief
Super Lemon Haze — Bright, Mood-First Relief
Super Lemon Haze Feminized Seeds (23% THC) leads with an intense limonene profile — more pronounced than almost any other common strain. For FM patients whose primary daytime struggle is depression, emotional flatness, and cognitive fog rather than physical pain alone, Super Lemon Haze addresses the neurological roots of mood dysregulation.
New York Power Diesel — High-Output Balanced Option
New York Power Diesel Feminized Seeds (24% THC) blends Sour Diesel's functional clarity with a slightly heavier body component from its Afghani genetics. It handles pain more aggressively than pure Sour Diesel while retaining enough mental clarity for daytime use — a practical middle-ground for FM patients with both significant pain and cognitive demands.
For Anxiety, Mood & Fibro Fog: Lower-THC, Terpene-Rich Strains
High THC content does not always equal better fibromyalgia outcomes — and for the anxiety and cognitive symptoms that affect roughly 30–40% of FM patients, lower-THC, terpene-rich options often outperform high-potency alternatives.
Cookies Kush — Caryophyllene-Forward Anti-Anxiety
Cookies Kush Feminized Seeds (18% THC) delivers the caryophyllene-dominant CB2 activation of OG Kush genetics at a THC level that is far less likely to trigger anxiety spirals. For FM patients whose cognitive symptoms worsen with high THC, this is a reliable entry point into indica-dominant relief.
Swiss Miss — The Low-THC Terpene Option
Swiss Miss Feminized Seeds (15% THC) sits at the lower end of the THC range in this catalog, making it ideal for fibromyalgia patients who are highly THC-sensitive — a common trait in FM. Lower THC with rich terpene expression (particularly in myrcene and humulene) provides the anti-inflammatory and mild analgesic effect without the risk of paradoxical pain amplification.
Microdosing for FM Sensitivity: Many fibromyalgia patients find more consistent relief from 2–3 mg THC taken every 4–6 hours than from a single large dose. Use a dry-herb vaporizer set to 170°C and take one single controlled draw per session — this delivers roughly 2–4 mg THC per draw from a well-packed chamber.
Strain Comparison at a Glance
| Strain | THC | Primary Terpenes | Best FM Target | Time of Day |
|---|---|---|---|---|
| Purple Kush | 27% | Myrcene, Linalool | Severe nighttime pain, sleep | Nighttime only |
| NL x Big Bud | 20% | Myrcene, Caryophyllene | Whole-body pain, sleep maintenance | Evening / night |
| Skywalker OG Auto | 23% | Caryophyllene, Myrcene | Pain + sleep, easy growing | Evening / night |
| Sour Diesel | 24% | Limonene, Caryophyllene | Daytime pain, mood, fatigue | Morning / midday |
| Super Lemon Haze | 23% | Limonene, Terpinolene | Depression, cognitive fog | Morning |
| NY Power Diesel | 24% | Limonene, Myrcene | Pain + mood balance | Daytime |
| Cookies Kush | 18% | Caryophyllene, Linalool | Anxiety, mild pain, fog | Afternoon / evening |
| Swiss Miss | 15% | Myrcene, Humulene | THC-sensitive patients, inflammation | Flexible |
Dosing Fibromyalgia Patients: Sensitivity, Titration & Avoiding Flares

Cannabis for fibromyalgia pain management requires a fundamentally different dosing approach than recreational use. FM patients consistently show heightened CNS sensitivity — the same neurological amplification that creates allodynia also makes them more reactive to THC's psychoactive and anxiogenic effects.
The guiding principle is "start low, go slow, stay low." This is not cautious timidity — it is pharmacologically accurate for a population with documented central sensitization.
Step-by-Step Titration Protocol for FM Patients
Start with CBD Alone (Days 1–7)
Begin with 15–25 mg CBD daily (oral), morning and evening. This establishes endocannabinoid tone via FAAH inhibition and anandamide elevation before introducing THC's direct receptor activity. Many FM patients notice sleep improvement within the first week from CBD alone.
Introduce Micro-Dose THC at Night (Week 2)
Add 2.5 mg THC via inhalation or oral preparation 60–90 minutes before bed. Do not increase daytime use at this stage. Monitor sleep quality, pain levels on waking, and any anxiety response over 5 days before adjusting.
Add Daytime THC if Night Dose Is Tolerated (Week 3)
Introduce 1–2 mg THC via vaporizer during the day — using a sativa-leaning or balanced strain. Limonene-dominant strains (Sour Diesel, Super Lemon Haze) at this dose range provide pain relief and mood lift with minimal sedation risk.
Titrate Upward Slowly and Track Results (Week 4+)
Increase either day or night dose by 2.5 mg THC per adjustment, with at least 72 hours between changes. Keep a symptom journal tracking pain (0–10), sleep quality (0–10), and mood. The effective dose for most FM patients plateaus between 10–25 mg THC/day total.
Maintain a Tolerance Break Cycle
Every 4–6 weeks, reduce THC by 50% for 3–5 days. Fibromyalgia patients who maintain a consistent high dose often experience diminishing analgesic returns as CB1 receptor downregulation develops. Brief tolerance breaks restore receptor sensitivity without prolonged withdrawal.
Flare Risk: Abrupt cannabis cessation in regular FM users can trigger a temporary pain and sleep flare lasting 24–72 hours as the endocannabinoid system readjusts. Taper down gradually rather than stopping cold. If you are also using opioids, always discuss cannabis introduction with your prescribing physician — interactions with CNS depressants require medical supervision.
Delivery Methods: Matching Administration to Fibromyalgia Symptoms

How you consume cannabis for fibromyalgia pain shapes the onset, duration, and intensity of relief as much as which strain you choose. Different delivery methods match different fibromyalgia symptom contexts — and mixing methods strategically can cover both acute pain spikes and baseline symptom management.
- Dry-herb vaporizer (170–185°C): Fastest onset (2–5 min), best for acute pain spikes and allodynia episodes. Preserves terpenes better than combustion. Ideal dose control via single-draw method. Best daytime option.
- Oral tinctures (sublingual): Onset 15–45 minutes, duration 4–6 hours. Better for sleep maintenance and baseline pain management. Most consistent dosing from a calibrated dropper. CBD:THC tinctures are the easiest format for precise ratios.
- Edibles/capsules: Slowest onset (45–90 min), longest duration (6–10 hours). Useful for patients who want overnight coverage. Highest variability in effect due to first-pass liver metabolism — 11-hydroxy-THC produced in the liver is significantly more potent than inhaled THC. Start at 2.5 mg and wait a full 2 hours before redosing.
- Topicals: Zero psychoactive effect, localized relief only. Excellent for focal allodynia, joint pain, and muscle tenderness. Apply CBD-dominant topicals directly to tender points. Won't affect brain-mediated central sensitization but reduce peripheral pain signals.
- Inhalation/smoking: Similar onset to vaporizing but destroys heat-sensitive terpenes and introduces combustion byproducts. Not recommended for FM patients who often have respiratory sensitivity.
For fibromyalgia, the most effective multi-symptom protocol combines a CBD-dominant tincture taken each morning and evening for baseline endocannabinoid support, a limonene-rich strain vaped during daytime pain episodes, and a myrcene-heavy indica vaped or in tincture form 60–90 minutes before sleep.
Growing Cannabis for Fibromyalgia: Consistency Through Home Cultivation

Patients who rely on cannabis fibromyalgia relief long-term face a persistent challenge: product consistency. Dispensary batches change, terpene profiles vary between harvests, and cost is a real barrier for a condition requiring ongoing daily use. Growing your own solves all three problems simultaneously.
For FM patients who may have limited physical energy, certain cultivation approaches are more practical than others. Autoflowering strains require no light schedule management and reach harvest in 70–85 days — significantly reducing the physical and cognitive demand of a grow. The autoflower vs. photoperiod guide covers the full comparison.
Best Growing Approaches for FM Patients
- Choose autoflowering feminized strains — no light schedule management required
- Use pre-amended living soil to minimize nutrient mixing and feeding schedules
- Set up an automated watering system — physical bending and lifting are FM flare triggers
- Grow 2–3 plants in a self-contained tent with integrated lighting and humidity control
- Select compact, bushy indica or indica-dominant genetics — easier canopy management
- Harvest at 30–40% amber trichomes for maximum CBN content and sedative effect
- Cure properly (minimum 4 weeks at 58% RH) to preserve therapeutic terpene profiles
Grow Tent Setup: A 60x60 cm tent with a 200W LED and automated coco-drip irrigation can produce 60–100 grams per autoflower with under 2 hours of hands-on time per week — realistic for FM patients managing energy budgets. See our complete indoor grow tent setup guide for a step-by-step walkthrough.
For harvest timing — which directly determines your THC-to-CBN ratio and therefore how sedating your final product is — see our guide on when to harvest cannabis for maximum potency. FM patients targeting sleep applications should harvest significantly later than patients targeting pain or mood.
Terpene preservation starts at harvest and ends in the jar. Our cannabis drying and curing guide covers the complete 2–8 week process — critical for ensuring that the myrcene and linalool you need for FM sleep benefits actually survive to your final product.
Avoiding Cannabis-Related Fibromyalgia Exacerbation

Cannabis is not universally beneficial for fibromyalgia — and a subset of patients experience worsened symptoms with specific products, doses, or patterns of use. Understanding the risk factors for exacerbation helps you course-correct quickly rather than abandoning a potentially effective treatment.
Patterns That Can Worsen FM Symptoms
- High-THC sativa strains in anxious patients: Limonene and terpinolene-dominant strains at high THC doses can amplify the sympathetic nervous system activation already elevated in many FM patients, triggering pain flares via central sensitization feedback
- Daily high-dose use without tolerance breaks: CB1 receptor downregulation reduces analgesic efficacy over 4–6 weeks of consistent high dosing, leading patients to escalate dose and diminish returns
- Heavy nighttime use disrupting REM sleep: THC suppresses REM sleep, which at low doses is benign — but at doses above 15–20 mg regularly, REM disruption begins to impair emotional processing and worsen next-day cognitive symptoms
- Combustion and smoke irritation: FM patients often have heightened mucosal sensitivity; smoking can trigger coughing fits that cause painful thoracic muscle spasms
- Cannabis hyperemesis in daily heavy users: Rare but documented; presents as cyclical nausea worsening FM quality of life — resolved by reducing use frequency
Drug Interaction Alert: Cannabis significantly enhances the CNS depressant effects of benzodiazepines, opioids, gabapentin, and pregabalin — all commonly prescribed in fibromyalgia management. Never begin cannabis use alongside these medications without explicit guidance from a prescribing physician. Combined use can cause respiratory depression at doses that would be safe individually.
Integrative Fibromyalgia Management: Cannabis as One Layer

The strongest clinical outcomes for fibromyalgia consistently emerge from multi-modal treatment programs — not single-intervention approaches. Cannabis fibromyalgia relief is most powerful when positioned as one layer of a broader symptom management strategy.
Current fibromyalgia management guidelines (American College of Rheumatology, 2022) emphasize aerobic exercise, cognitive behavioral therapy (CBT), sleep hygiene protocols, and stress reduction as first-line interventions — all of which can be meaningfully supported by thoughtful cannabis use rather than competing with it.
How Cannabis Supports (Rather Than Replaces) Other FM Treatments
- Exercise: Low-dose daytime cannabis reduces the exercise-induced pain amplification that keeps many FM patients sedentary — making movement more accessible without eliminating its therapeutic benefit
- Sleep hygiene: Cannabis addresses the physiological sleep disruption (poor slow-wave sleep) that behavioral protocols alone cannot fully correct in central sensitization
- CBT / mindfulness: CBD's anxiolytic effect and THC's sensory modulation can lower baseline anxiety enough for patients to engage more fully with psychological interventions
- Physical therapy: Topical CBD applied to tender points before PT sessions may reduce localized allodynia enough to allow deeper work on muscle deactivation patterns
- Dietary anti-inflammatory protocols: Cannabis reduces neuroinflammatory markers — synergistic with omega-3 and polyphenol-rich dietary approaches targeting systemic inflammation
For FM patients also dealing with muscle spasms — a common comorbid symptom — our dedicated guide on best cannabis strains for muscle spasms and tension relief covers complementary strain selections targeting this specific symptom.
Cannabis does not cure fibromyalgia. No current treatment does. What well-chosen cannabis can do is reduce the barrier to other therapeutic activities — making exercise less painful, sleep more restorative, and emotional regulation more accessible — which compound over time into meaningful quality-of-life gains.
The entourage effect is especially relevant in integrative FM management: full-spectrum preparations that preserve the whole cannabinoid and terpene profile consistently outperform isolated THC or CBD alone in clinical surveys, precisely because fibromyalgia's multi-system dysfunction requires multi-target pharmacology.
Frequently Asked Questions

What is the best cannabis strain for fibromyalgia pain?
There is no single best strain for fibromyalgia — the optimal choice depends on which symptom cluster dominates. For nighttime pain and sleep, indica-dominant strains with high myrcene content like Purple Kush (27% THC) or Northern Lights x Big Bud (20% THC) perform best. For daytime pain with mood support, limonene-rich sativa-leaning strains like Sour Diesel (24% THC) or Super Lemon Haze (23% THC) are more appropriate. Most FM patients benefit from using different strains at different times of day rather than relying on one product for all symptoms.
Is CBD or THC better for fibromyalgia?
Both cannabinoids play distinct roles in fibromyalgia management, and the research consistently shows balanced THC:CBD ratios outperform either alone for pain relief. THC directly modulates CB1 receptors in pain-processing brain regions and promotes slow-wave sleep. CBD raises anandamide levels via FAAH inhibition, reducing central sensitization and anxiety. A 1:1 CBD:THC ratio is the most studied combination for chronic pain. For fibro fog and anxiety, CBD-dominant preparations (4:1 CBD:THC) are preferred; for sleep onset, THC-dominant formulations work faster.
What does research say about cannabis for fibromyalgia?
Published fibromyalgia cannabis studies, including a significant 2018 Israeli observational study of 367 patients, show 81% reported meaningful pain improvement and over 50% reduced opioid use after 6 months of medical cannabis. A 2019 crossover trial found vaporized balanced THC:CBD produced the greatest analgesic effect. Synthetic THC (nabilone) demonstrated significant pain and quality-of-life improvement in a double-blind RCT (Skrabek et al., 2008). Current evidence is primarily observational rather than from large RCTs, but is consistent enough that many rheumatology specialists now consider cannabis a reasonable adjunct therapy.
Why are fibromyalgia patients more sensitive to THC?
Fibromyalgia is a central sensitization disorder — the nervous system is already in a state of amplified reactivity. This same amplification extends to THC's psychoactive and anxiogenic effects. FM patients frequently report that doses tolerated easily by healthy individuals trigger anxiety, tachycardia, or paradoxical pain intensification. This is why the standard recommendation is to begin at 2.5 mg THC and increase by no more than 2.5 mg per adjustment, with at least 72 hours between dose changes. Lower-THC strains (15–20% range) with rich terpene profiles are often more therapeutically effective than maximal-potency options.
Can I grow my own cannabis for fibromyalgia at home?
Yes — home cultivation is a practical and cost-effective approach for FM patients requiring consistent, long-term cannabis access. Autoflowering feminized strains are the most accessible option because they require no photoperiod management and reach harvest in 70–85 days. Skywalker OG Autoflower (23% THC), Cookies Kush Feminized (18% THC), and Blue Moonshine Autoflower (13% THC) are among the most manageable options for patients with limited physical energy. A small automated grow tent with pre-amended living soil can produce 60–100g per plant with under 2 hours of hands-on time per week. Always verify local cultivation laws before growing.